- The nose is the central feature of the face. Its aesthetics affect the rest of the facial features in several ways.
- Many techniques have been described which help improve the appearance of the nose. None of these are as versatile as a proper open rhinoplasty.
- To fully appreciate rhinoplasty, it is essential to have a good understanding of the anatomy of the nose and the recommended aesthetic proportions.
CONTENTS
- Anatomy of the Nose
- Aesthetic Proportions of the Nose
- Cosmetic and Functional Rhinoplasty
- How Rhinoplasty Changes the Whole Face
- Closed vs Open Rhinoplasty
- Minimally Invasive Technique vs Closed vs Open Rhinoplasty
ANATOMY OF THE NOSE
 Anatomy of Nasal bone and Cartilages
Anatomy of Nasal bone and Cartilages- The nose can be divided into thirds :
- Upper third of the nose is made up of the nasal bones
- Low bony radix is a common complaint
- Middle third is occupied by the upper lateral cartilages which join the nasal septum. This septum separates the left and right nostrils
- Lower third is occupied by the lower lateral cartilages
- A low dorsum and broad nasal tip is due to a small and short nasal septum with weak and broadened lower lateral cartilages.
- Upper third of the nose is made up of the nasal bones
AESTHETIC PROPORTIONS OF THE NOSE
- The important aesthetic proportions of the nose originally described for Caucasian still applies to the Oriental nose.
- The followings are selected features which are applicable in Oriental rhinoplasty
FRONT VIEW
 Facial proportion – Rhinoplasty
Facial proportion – Rhinoplasty Facial proportion – Side – Rhinoplasty
Facial proportion – Side – Rhinoplasty- Face is divided into upper, middle and lower thirds at (i) hairline, (ii) brow at the level of the supraorbital notch, (iii) subnasale, and (iv) mentum.
- Lower third is further divide into (1) upper third and (2) lower two thirds by line between oral commissures.
 Face Proportion – Nose Width – Rhinoplasty
Face Proportion – Nose Width – Rhinoplasty- The width for the nose is equal to one eye width (intercanthal distance).
LATERAL VIEW
 Facial proportion – Length of Nose – Rhinoplasty
Facial proportion – Length of Nose – Rhinoplasty- Tip projection :
- The ratio of nasal length to tip projection should be 1.0:0.67 or 3:2 (Bryd).
 Facial proportion – Columellar labial angle – Rhinoplasty
Facial proportion – Columellar labial angle – Rhinoplasty- Columellar-labial angle is at the junction of the columella with the upper lip.
- The aesthetic columellar-labial angle is 90-95o for male and 95-105o for female.
AESTHETIC PROPORTIONS OF THE CHIN
 Facial Proportion – Chin – Rhinoplasty
Facial Proportion – Chin – Rhinoplasty- It is very important to have chin length and projection proportional to that of the nose.
- The Riedel’s plane is a simple way to assess the aesthetics of the chin. It is a line connecting the most prominent portion of the upper and lower lip which, on a balanced face, should touch the most prominent anterior portion of the chin (pogonion).
COSMETIC AND FUNCTIONAL RHINOPLASTY
- Rhinoplasty can be done for cosmetic and reconstructive purposes.
- Cosmetic rhinoplasty addresses the followings :
- Low nasal dorsum and radix
- Wide nasal vault
- Poor tip projection
- Broad nasal tip
- Broad alar
- Poor columellar projection
- Short nose
- Crooked nose
- Functional rhinoplasty treats the followings :
- Functional and structural deformities
- Cleft lip and palate nasal deformity
- Septal perforation
- Nasal passage obstruction due to nasal valve dysfunction
- Inferior turbinate hypertrophy
- Deviated septal bones
- Nasal tumor
- Traumatic incidence such as sports injury, fall, road traffic accident etc
- Post traumatic event resulting in deviated septum and/or dorsum; facial fracture
- Deformities caused by previous rhinoplasty
- Functional and structural deformities
HOW RHINOPLASTY CHANGES THE WHOLE FACE
- A well augmented nose can improve the other facial features in many ways :
- Gives the face a more three-dimensional and slimmer appearance.
- Reduce the distance of the inner corner of the eye (medial epicanthoplasty effect), making the eye appear longer
- Improve the columellar-labial angle :
- This can make a patient look younger especially when if the upper lip is receded (giving an illusion of aged appearance).
- Improve the nasolabial fold
- Improve the columellar-labial angle :
METHODS OF NOSE AUGMENTATION
- There are various methods to augment the nose:-
- Minimally Invasive Techniques :
- Hyaluronic acid filler injection
- Fat injection to nose
- Thread insertion
- Closed Rhinoplasty :
- This is a smaller procedure with no external scar. It has limited capabilities and its effects are not as dramatic as open rhinoplasty.
- Open Rhinoplasty :
- This has been the de-facto standard for performing Oriental rhinoplasty in many countries especially in South Korea.
- It allows full visualisation of all internal structures of the nose and enables a full range of corrective procedures to be done with accuracy.
TABLE OF COMPARISON OF CLOSED VS OPEN RHINOPLASTY
| Closed Rhinoplasty | Open Rhinoplasty | |
|---|---|---|
| Diagram |  Closed Rhinoplasty – Incision Closed Rhinoplasty – Incision |  Open Rhinoplasty – Incision Open Rhinoplasty – Incision |
| External Scar | Incision within the nose with no external scar. | Small imperceptible scar across the columella. The rest of the scar is within the nose. |
| Visualisation of Internal Structures of Nose | Limited visualisation through a small opening. | Complete visualisation of all structures of the nose – allows accurate diagnosis and surgical correction. Accurate placement of implant or cartilage graft. |
| Corrective Capability | Limited range of corrective procedures. Difficult to suture and secure implants or cartilage grafts in position. | Full range of corrective surgery can be done. Position of implant or cartilage graft is visually confirmed and secured in place with suturing |
| Duration of Surgery | Shorter | Longer |
| Post-op Recovery | Usually shorter. Most swelling and bruising subside in 1-2 weeks. Most patients return to work in 1-2 weeks. | Slightly longer recovery. Significant decrease in swelling and bruising in 2 weeks. Most patients return to work in 1-2 weeks. |
TABLE OF COMPARISON CAPABILITIES OF MINIMALLY INVASIVE TECHNIQUE VS CLOSED VS OPEN RHINOPLASTY
- This table outlines the common problems in the Oriental nose and their corrective measures.
| Minimally Invasive e.g Filler | Closed Rhinoplasty | Open Rhinoplasty | |
|---|---|---|---|
| Low dorsum Low radix | Slight improvement to dorsum and radix height. (excessive filler material can result in a broad radix) |  Insertion silicone implant (usually L-shaped) | Insertion of silicone implant or rib cartilage. (Less tendency for implant displacement because of more accurate placement and ability to suture the implant in place) |
| Wide nasal vault | Unable to correct. | Unable to correct. |   Nasal bone narrowed by :
|
| Poor tip projection | Can improve tip projection slightly but cannot refine the tip. | Insertion of L-shape implant to improve tip projection. (High risk of implant perforation to the skin) | 
|
| Broad nasal tip | Unable to correct. | Unable to correct a broad nasal tip well. | Tiplasty (suturing of the nasal cartilage to produce a more refined tip) |
| Broad alar | Unable to correct. | Alarplasty can be combined with closed rhinoplasty |  Rhinoplasty – Alarplasty Rhinoplasty – AlarplastyOpen rhinoplasty can produced better tip projection thereby reducing the need for alarplasty. |
| Poor columellar projection | Difficult to achieve | Insertion of L-shape implant to improve columellar projection. (usually limited results) | Caudal extension graft to improve columellar projection. |
| Short nose | Unable to correct. | Insertion of L-shape implant to increase nasal line. (usually limited results) | Caudal extension graft to improve length of nose. |
| Crooked nose | Illusion of improvement but not actually correcting the nasal anatomy. | Unable to correct. | Osteotomy is cutting of the nasal bone (osteotomy) and rasping (filing of the nasal bone) |
| Septal deviation and nasal obstruction | Unable to correct. | Limited septoplasty. |
|


TYPE OF CARTILAGE GRAFT USED IN RHINOPLASTY
| Origin | Ear | Nose(Septum) | Chest(Rib) |
|---|---|---|---|
| Autogenous cartilage graft | Conchal cartilage | Septal cartilage | Costal cartilage |
| Diagram | 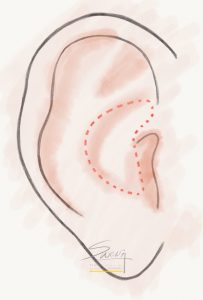 Rhinoplasty – Conchal (Ear) Cartilage Harvest Rhinoplasty – Conchal (Ear) Cartilage Harvest |  Rhinoplasty – Septal cartilage graft Rhinoplasty – Septal cartilage graft | 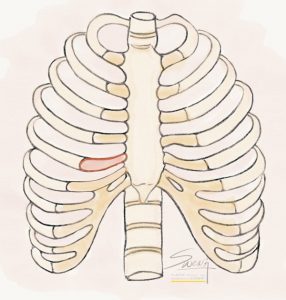 Rhinoplasty – Rib Cartilage Graft Rhinoplasty – Rib Cartilage Graft |
| Characteristic | Curved, flexible cartilage, shaped like a bowl. |
|
|
| Function |
|
|
|