WHAT IS FAT GRAFTING?
- The ageing process is characterised by:
- Loss of elastic components of the skin e.g. collagen and elastin fibres
- Loss of volume due to loss of fat and dermis thickness.
- This result in a saggy and sunken appearance, which is more indicative of ageing than wrinkles alone.
- Anti-ageing treatment aims to:
- Improve skin elasticity e.g. Laser resurfacing, Profractional laser, infra-red therapy (Sciton SkinTyte) radiofrequency and high powered focused ultrasound.
- Restore lost volume e.g. hyaluronic acid filler injection and fat grafting or injection.
- Terminology:
- Fat injections, fat grafting and fat transfer surgery are essentially synonymous.
Fat Grafting Vs Filler Injection
| | Fat Grafting or Injection | Filler Injection |
|---|
| 1 | Material injected | Patient’s own fat | Hyaluronic acid – pre-manufactured |
| 2 | Process | Fat is harvested from the patient and separated into 3 layers by spinning in a centrifuge | No processing needed |
| 3 | Injection Technique | Injections are done in small aliquots (parcels) neatly in a row or rows to allow maximal surface area for absorption of blood and oxygen. The injected fat is not massaged to prevent damaging the fat. | Usually from a single injection point. Filler is injected in a “blob” and distributed more evenly by massaging the skin surface after the injection. |
| 4 | Volume of injection | Usually larger volume for subtle improvement of various facial features and volume restoration | Usually small volume replacement |
| 5 | Post-op appearance | Bruising and swelling significantly reduced after 1-2 weeks. | Bruising and swelling for up to a week |
| 6 | Duration of result | About 60-70% of the injected fat cells would eventually survive and stay permanently. The final result is seen in 2-3 months. | Most hyaluronic acid filler is gradually absorbed by the body in about 6 months. |
| 7 | Cost effectiveness | More cost effective when large volume is needed e.g. 5-6 ml onwards. | Not cost effective for large volume replacement. |
Sites of Fat Grafting Surgery include
- Face
- Breast
- Scar
- Wounds with delayed healing
- Studies have shown improved wound healing after fat injection to non-healing wounds due to the small amount of adipose (fat) derived stem cells present.
Fat Grafting to Face:
- For anti-ageing purpose: Temporal area, upper and lower eyelid, nasolabial fold and Marionette line
- For contour deficiency and to improve the 3-dimensional profile of the face: e.g. forehead and chin
- Scarring:
- There are usually a few needle puncture marks which heal without scarring.
Fat Grafting to Breast:
- Purpose:
- Alternative to breast augmentation using breast implant:
- Improve the shape of sagging breast
- Restore contour irregularity after previous breast surgery.
- Important technical points:
- It is absolutely important to inject the fats only into the subcutaneous layer (skin layer) of the breast and NOT into the actual breast parenchyma (the breast tissue that is capable of milk production).
- It is also possible to inject the fats just above the pectoralis major muscle (chest muscle). However this is difficult to achieve accurately and may risk puncturing the lungs.
- Mammography after fat grafting to breast:
- Not all the fat injected will survive. Most non-surviving fats cells are completely absorbed by the body. Some of these may leave behind minute amount of calcium deposits. This pattern of calcium deposition is called “macro-calcification”. This is different from the “micro-calcification” pattern shown on mammogram characteristic of breast cancer.
- In the past radiologist have difficulty differentiating between the two patterns of calcification. Nowadays, most of them are able to tell them apart.
- Volume retention:
- The potential volume transferrable depends on how much fat reserve a patient has for harvesting. Therefore it is not possible to transform from “A” to “C” cup if the patient has hardly any fat reserve.
- In general it is possible to increase half to one cup size in each fat grafting session.
- Scarring:
- There are usually one to two (less than 5 mm) puncture marks which heal without noticeable scarring.
Fat Grafting to Scar:
- Purpose:
- Fill up volume deficit for sunken (atrophic) scar
- Improve the skin texture of scar
SUITABLE CANDIDATES FOR FAT TRANSFER AND FAT GRAFTING SURGERY
- Most people have sufficient fat reserves for the grafting procedure.
DESCRIPTION OF FAT TRANSFER AND FAT GRAFTING PROCEDURE
PROCESS OF FAT GRAFTING (COLEMAN TECHNIQUE)
- Modern day fat grafting procedures are largely modelled after the technique of structural fat grafting pioneered by Dr Sydney Coleman.
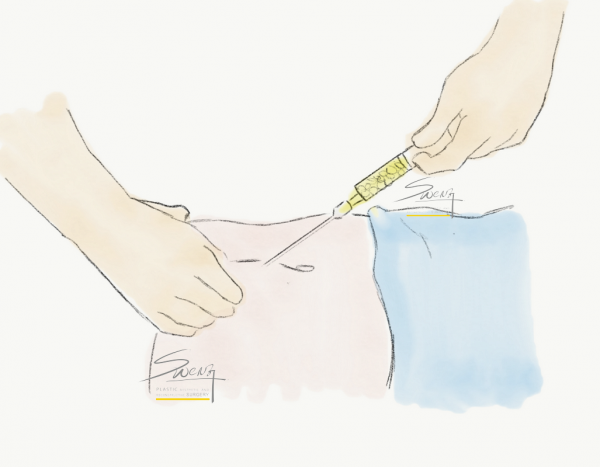
Fat harvesting from via a small puncture
Fat Harvesting:
- The donor sites are usually the abdomen, thighs or buttocks.
- Fat is harvested using a 10 ml syringe via a small cut (less than 5 mm). This process is manual and it is very important to be gentle to minimise damage to the fat cells.
- The fat obtained from an actual liposuction procedure is not of the best quality. This is because the liposuction process uses a vibrating mechanical device which induces mechanical trauma to the fat cells.
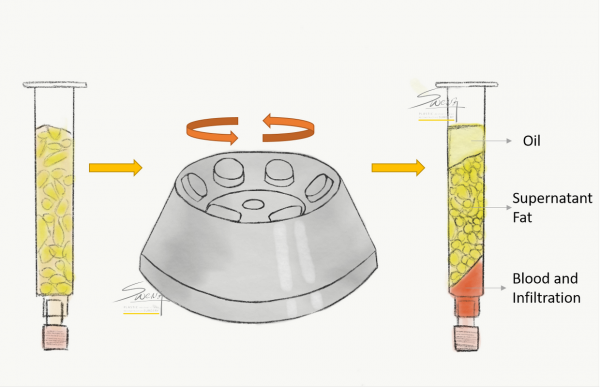
Centrifugation to separate fats harvested into three layers
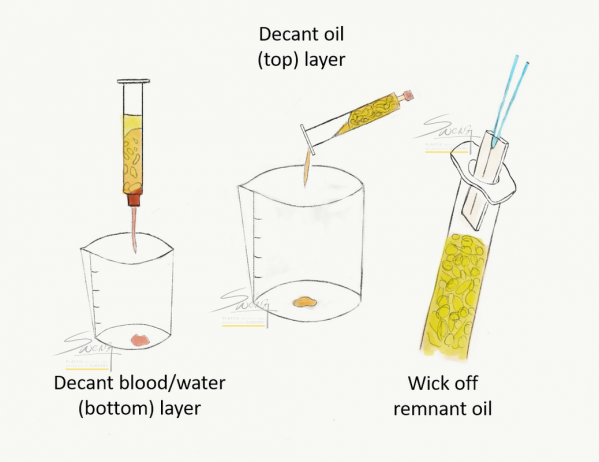
Purifying fat by removal of unnecessary component before grafting
Fat Processing:
- The harvested fat is then centrifuged to separate it into 3 layers: (1) top layer of oil from broken fat cells, (2) middle layer of usable fat cells, and (3) bottom layer of blood and water.
- The top and bottom layers are discarded. The middle layer is used for injection.
- The middle layer of fat cells is transferred carefully into 1 ml syringes for injection.
- There are other systems available for fat processing. However, some may risk contamination of the fat.
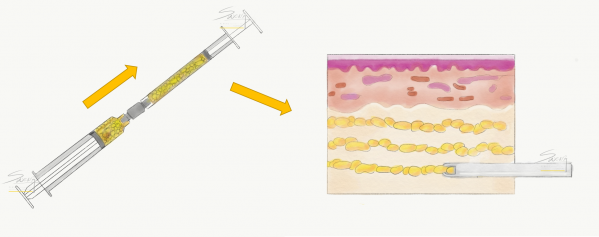
Fat injection in small parcels in layers to ensure maximal survival
Fat Injections:
- The fat is injected in small parcels (aliquots) in multiple layers to ensure even distribution and to allow maximal surface area for the fats cells to absorb blood and oxygen from the surrounding tissue to improve survival.
- It is best to use 1 ml syringes which allow accurate control of this injection process.
- Therefore, injecting 100 ml would require the use of many of these syringes.
FAT SURVIVAL AFTER FAT GRAFTING
With proper techniques by an experienced fat transfer plastic surgeon in Singapore, at least 60-70% of the injected fat cells would survive. These would yield permanent results.
The following are best practices to improve fat survival:
- Careful aspiration of fat by hand using low suction power.
- Centrifugation to separate the fat cells from the unwanted fluid
- Careful injection in small parcels in multiple layers to ensure maximal fat cell survival.
- Avoid over injection which would increase tissue pressure and reduce blood flow and hence fat cell survival.
PROCEDURES DONE TOGETHER WITH FAT GRAFTING
Fat grafting can be done in association with the following procedures:
- Facelift
- Upper eyelid surgery
- Eyebag removal
- Breast Augmentation
- Scar revision
- A patient undergoing liposuction of the abdomen and thighs may transfer the unwanted fat to the breasts
- A Mummy makeover which consists of a tummy tuck and breast augmentation. Fat transfer to the breast can be considered instead of breast implant.
- Fat transfer to face and breast concurrently.
ANAESTHESIA
- It can be done under local anaesthesia, a combination of local anaesthesia and sedation or general anaesthesia, depending on the volume to be transferred.
POST OPERATIVE CARE
- Day surgery procedure; home on the same day.
- Mild discomfort and ache over fat donor site – relieved by painkiller.
- Swelling and bruising are usually resolved within two weeks of recuperation.
- Avoid exertion and when resting, raised the affected body part upright to 30 degrees for optimal recovery.
- Avoid pressure over the fat grafted area to ensure optimal survival.
RISK AND COMPLICATION OF FAT TRANSFER SURGERY
- Bruising and swelling are within expectation and are usually resolved within two weeks.
- Uneven fat absorption, and asymmetry
- Macrocalcification e.g. in the breast
COST OF FAT GRAFTING
- Fat grafting is usually done for cosmetic reasons and therefore not insurance claimable.
- The exception would be when this is done as part of a reconstructive surgery to restore contour irregularity.
FREQUENTLY ASKED QUESTIONS
Why do I hear more about filler injection than Fat grafting or injection?
The majority of patient requests are for small volume injections. This is achieved by hyaluronic acid filler which can be administered by plastic surgeons, dermatologists and aesthetic physicians.
A minority of patients are aware of the potential of using fat grafting for rejuvenation and improvement of the contour of their whole face. A limited number of plastic surgeons perfrom fat grafting compared to doctors administering fillers.
When should I choose filler injection?
Filler is suitable when you need only a small volume replacement e.g. nasolabial fold (which typically requires 1-2 ml of filler). It is a quick and convenient treatment.
When should I consider fat grafting?
Fat grafting is more cost effective when larger volume replacement is needed e.g. more the 5-6 ml of volume replacement or full face volume replacement. The result is permanent.
Who are the candidates who choose breast augmentation using fat grafting rather than breast implant?
The candidates who opt for fat grafting to the breast would insist on the most natural result, without the risk of implant capsular contracture and implant rupture. They are willing to undergo multiple fat grafting sessions to achieve the desired volume.
Why do some people complain of complete fat loss after fat grafting?
There is almost always some fat retention after fat grafting. However poor fat survival rate can occur if the best practices for fat grafting, as discussed above, are not followed. Also, there is a substantial amount of swelling after fat grafting. When this swelling resolves over weeks to months gradually, some patients have a false impression that all the volume has been lost.
As one of the best fat grafting surgeons in Singapore, Dr. Ng will customise the most suitable strategy for rejuvenation and volume filling for you, during the consultation. This could include fat grafting (transfer), face lift procedures and laser resurfacing and skin tightening. A combination of procedures to achieve a harmonious result is commonly recommended by top plastic surgeons in Singapore and around the world.

 Open Technique of forehead lump removal
Open Technique of forehead lump removal Forehead Lump Removal - no visible scar") Endoscopic (Scarless) Forehead Lump Removal – no visible scar
Endoscopic (Scarless) Forehead Lump Removal – no visible scar Breast Reconstruction
Breast Reconstruction Pedicled TRAM flap harvest after mastectomy for immediate breast reconstruction
Pedicled TRAM flap harvest after mastectomy for immediate breast reconstruction TRAM flap placed inset into the remnant breast skin envelop – Best breast reconstruction method
TRAM flap placed inset into the remnant breast skin envelop – Best breast reconstruction method Breast Reconstruction – TRAM Flap – Post operative appearance with drains – Best breast reconstruction method
Breast Reconstruction – TRAM Flap – Post operative appearance with drains – Best breast reconstruction method Flap for Breast Reconstruction - alternative top option breast cancer surgery") Latissimus Dorsi (LD) Flap for Breast Reconstruction – alternative top option
Latissimus Dorsi (LD) Flap for Breast Reconstruction – alternative top option Breast Implant and Tissue Expander for Breast Reconstruction – Single stage or two stage reconstruction
Breast Implant and Tissue Expander for Breast Reconstruction – Single stage or two stage reconstruction Breast Reconstruction Timeline – recommended schedule for best possible result
Breast Reconstruction Timeline – recommended schedule for best possible result Coolsculpting – Cryolipolysis – Mechanism
Coolsculpting – Cryolipolysis – Mechanism Coolsculpting – Cryolipolysis – Body – Front
Coolsculpting – Cryolipolysis – Body – Front Coolsculpting – Cryolipolysis – Body – Back
Coolsculpting – Cryolipolysis – Body – Back Anatomy of Nasal bone and Cartilages
Anatomy of Nasal bone and Cartilages Facial proportion – Rhinoplasty
Facial proportion – Rhinoplasty Facial proportion – Side – Rhinoplasty
Facial proportion – Side – Rhinoplasty Face Proportion – Nose Width – Rhinoplasty
Face Proportion – Nose Width – Rhinoplasty Facial proportion – Length of Nose – Rhinoplasty
Facial proportion – Length of Nose – Rhinoplasty Facial proportion – Columellar labial angle – Rhinoplasty
Facial proportion – Columellar labial angle – Rhinoplasty Facial Proportion – Chin – Rhinoplasty
Facial Proportion – Chin – Rhinoplasty Closed Rhinoplasty – Incision
Closed Rhinoplasty – Incision Open Rhinoplasty – Incision
Open Rhinoplasty – Incision





 Rhinoplasty – Alarplasty
Rhinoplasty – Alarplasty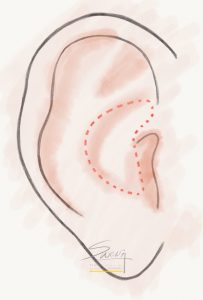 Rhinoplasty – Conchal (Ear) Cartilage Harvest
Rhinoplasty – Conchal (Ear) Cartilage Harvest Rhinoplasty – Septal cartilage graft
Rhinoplasty – Septal cartilage graft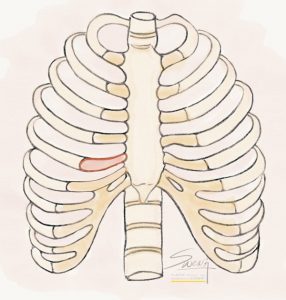 Rhinoplasty – Rib Cartilage Graft
Rhinoplasty – Rib Cartilage Graft Labiaplasty – Trim
Labiaplasty – Trim Labiaplasty – Wedge Excision
Labiaplasty – Wedge Excision Labiaplasty – Z Plasty
Labiaplasty – Z Plasty Labiaplasty – De-epithelialization
Labiaplasty – De-epithelialization Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis
Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis Blepharoptosis
Blepharoptosis Dermatochalasis
Dermatochalasis Blepharoptosis Assessment – MRD
Blepharoptosis Assessment – MRD Ptosis Assessment by Coverage of Limbus
Ptosis Assessment by Coverage of Limbus Blepharoptosis Assessment by MRD
Blepharoptosis Assessment by MRD Levator Function Test – Lid Closed
Levator Function Test – Lid Closed Levator Function Test – Lid Open
Levator Function Test – Lid Open Caucasian Double Eyelid vs Oriental Single Eyelid
Caucasian Double Eyelid vs Oriental Single Eyelid Suture Blepharoplasty
Suture Blepharoplasty Suture blepharoplasty – Cross section
Suture blepharoplasty – Cross section Incisional Blepharoplasty
Incisional Blepharoplasty Upper Eyelid – High Tapered fold – Blepharoplasty
Upper Eyelid – High Tapered fold – Blepharoplasty Upper eyelid – Parallel fold – Blepharoplasty
Upper eyelid – Parallel fold – Blepharoplasty Upper eyelid – Low in-fold – Blepharoplasty
Upper eyelid – Low in-fold – Blepharoplasty - Double eyelid surgery") Eyelid – Tapered fold (high)
Eyelid – Tapered fold (high)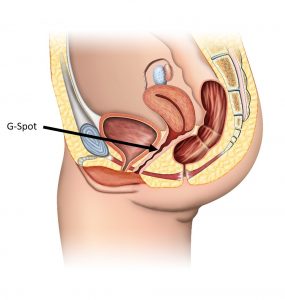 G-spot Location
G-spot Location