Advancements in medical science, technology and techniques have made cosmetic surgery safer, more effective and the results more natural-looking.
Surgery is the gold standard for facial rejuvenation and imparts the most lasting and dramatic results. Since the 1900s, facelifts have been used to reduce the appearance of sagging skin, iron out wrinkles, tighten and return shape to the brow, cheek and jaw and lift loose folds in the neck.
Since then, surgical facelift procedures have advanced by leaps and bounds. There are many surgical options to choose from – each addressing a specific area of the face and neck. Techniques have also become more refined and safe, with less scarring and quicker healing.
Types of lift
The areas that droop with age include the brow, mid-cheek, lower cheek and neck. There
are several types of facelifts available and the choice of procedure depends on the issues to be addressed and the extent of skin laxity. It is ideal to perform conventional facelift with a neck lift or browlift for a more harmonious result.
Conventional facelift
A conventional facelift is ideal for older people or those with severe laxity. There are several classifications and terminologies which are often confusing to the patient. In a long scar full facelift, the incision starts from the temporal area, passing in front of the ear and curving backwards behind it. A short scar face lift dispenses with the temporal incision and minimises the cut behind the ear. The longer the incision, the greater amount of laxity to be addressed.
The skin is then separated from the underlying tissue layer (called SMAS), redraped and shifted. The SMAS layer
is sutured to provide strength to the lift and any excess skin is trimmed. This type of facelift is the longest lasting and achieves the most dramatic results.
In recent times there has been great interest in the mini facelift. This involves a shorter scar, less tissue separation, reduced swelling and bruising, and shorter downtime. The result may not be as drastic as a full facelift, and most patients can return to work within one to two weeks after the procedure.
Browlift
A brow lift corrects sagging skin in the forehead, upper eyelids, and eyebrows. Also called a forehead lift, the procedure restores the appearance by correcting a heavy, sagging brow, and smoothing out deep furrows, to the upper third of the face. It is usually done with the use of an endoscope via several small incisions behind the hairline. The forehead skin is lifted and secured with sutures fixed to the skull. The result greatly complements a facelift.
Threadlift
Patients with mild skin laxity and redundancy may opt for a less invasive threadlift procedure. Threadlifts last for up to two years and are repeatable as new threads can be attached or existing ones adjusted.
The procedure is done under local anaesthetic and sedation and involves placing specially designed surgical threads under the skin in different positions using a thin needle. These implanted threads have barbs or cones which are pulled in different directions to lift the sagging skin. Side-effects include bruising and swelling which may resolve within a week.
Non-invasive lifting procedures
Minimally invasive or non-surgical facelifts are increasingly popular though they do not offer the same results. They are a good option for those who do not wish to undergo surgery. They generate heat damage to the collagen in the deep dermis resulting in regeneration and lifting. Some of these treatments are based on infrared, focused ultrasound and radio frequency.
Filler injection has been inappropriately termed as a face lifting procedure. Strictly speaking, a lifting procedure is anti-gravity and has a single direction of pull with stable fixation of tissue. Fillers provide generalised multi-directional distension of tissue with volumisation effect.
There is no ‘right’ or ideal procedure as it all depends on an individual’s desired results, the shape of his or her face and the extent of laxity. It is important to speak with your surgeon on the most suitable procedure appropriate for your unique case.
 Anatomy of Nasal bone and Cartilages
Anatomy of Nasal bone and Cartilages Facial proportion – Rhinoplasty
Facial proportion – Rhinoplasty Facial proportion – Side – Rhinoplasty
Facial proportion – Side – Rhinoplasty Face Proportion – Nose Width – Rhinoplasty
Face Proportion – Nose Width – Rhinoplasty Facial proportion – Length of Nose – Rhinoplasty
Facial proportion – Length of Nose – Rhinoplasty Facial proportion – Columellar labial angle – Rhinoplasty
Facial proportion – Columellar labial angle – Rhinoplasty Facial Proportion – Chin – Rhinoplasty
Facial Proportion – Chin – Rhinoplasty Closed Rhinoplasty – Incision
Closed Rhinoplasty – Incision Open Rhinoplasty – Incision
Open Rhinoplasty – Incision





 Rhinoplasty – Alarplasty
Rhinoplasty – Alarplasty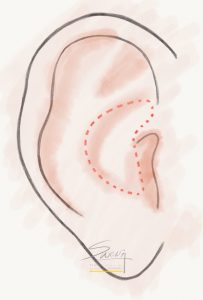 Rhinoplasty – Conchal (Ear) Cartilage Harvest
Rhinoplasty – Conchal (Ear) Cartilage Harvest Rhinoplasty – Septal cartilage graft
Rhinoplasty – Septal cartilage graft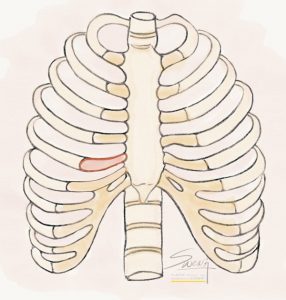 Rhinoplasty – Rib Cartilage Graft
Rhinoplasty – Rib Cartilage Graft Labiaplasty – Trim
Labiaplasty – Trim Labiaplasty – Wedge Excision
Labiaplasty – Wedge Excision Labiaplasty – Z Plasty
Labiaplasty – Z Plasty Labiaplasty – De-epithelialization
Labiaplasty – De-epithelialization Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis
Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis Blepharoptosis
Blepharoptosis Dermatochalasis
Dermatochalasis Blepharoptosis Assessment – MRD
Blepharoptosis Assessment – MRD Ptosis Assessment by Coverage of Limbus
Ptosis Assessment by Coverage of Limbus Blepharoptosis Assessment by MRD
Blepharoptosis Assessment by MRD Levator Function Test – Lid Closed
Levator Function Test – Lid Closed Levator Function Test – Lid Open
Levator Function Test – Lid Open Caucasian Double Eyelid vs Oriental Single Eyelid
Caucasian Double Eyelid vs Oriental Single Eyelid Suture Blepharoplasty
Suture Blepharoplasty Suture blepharoplasty – Cross section
Suture blepharoplasty – Cross section Incisional Blepharoplasty
Incisional Blepharoplasty Upper Eyelid – High Tapered fold – Blepharoplasty
Upper Eyelid – High Tapered fold – Blepharoplasty Upper eyelid – Parallel fold – Blepharoplasty
Upper eyelid – Parallel fold – Blepharoplasty Upper eyelid – Low in-fold – Blepharoplasty
Upper eyelid – Low in-fold – Blepharoplasty - Double eyelid surgery") Eyelid – Tapered fold (high)
Eyelid – Tapered fold (high)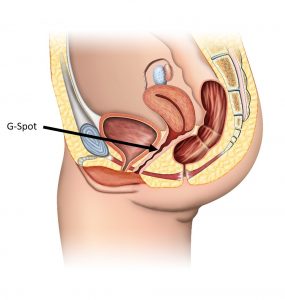 G-spot Location
G-spot Location