The quest for youth has spurned a multi-billion dollar industry. Today, the multitude of rejuvenation options is bewildering. A person’s choice of rejuvenation technique is generally determined by his or her physical state, tolerance for pain and downtime, and financial constraints.
The clinical problems that we commonly address include pigmentation, superficial textural imperfections, wrinkles (dynamic or static), deep folds or contour deformities, and skin laxity.
Rejuvenation options are divided broadly into non-invasive (non-surgical) and invasive (surgical) procedures with a few options in the “borderline” zone. Patients should be aware that all these rejuvenation techniques have a common goal of causing controlled damage to the various layers of the skin in order to stimulate repair and regeneration. Sun avoidance and strict usage of sunscreen are the keys to maintaining the results and preventing hyperpigmentation.
NON-INVASIVE (NON-SURGICAL) PROCEDURES
The most common form of phototherapy treatment is Intense Pulsed Light (IPL) or Broadband Light (BBL), which is able to improve the general complexion, lighten pigmentation, improve fine wrinkles and mildly tighten the skin. It is also effective for permanent hair removal. IPL/BBL is a suitable option for regular maintenance without downtime.
To achieve further textural improvement to the superficial layer of the skin, laser resurfacing is more effective. Erbium Yag lasers or carbon dioxide lasers are commonly used to ablate a thin epidermal layer. Erbium Yag is more suited for Asian skin types than carbon dioxide laser. The treated area will be raw and require regular application of antibiotics; the downtime for microlaser peel is around 3 to 5 days, after which a patient can resume putting on makeup.
Various treatment modalities are available to further tighten the dermal layer to for lifting and improvement of static wrinkles. Profractional Erbium Yag (or carbon dioxide) laser, radiofrequency, focused ultrasound and infrared waves can be used to cause thermal injury to the dermal collagen and elastin in a controlled manner. This induces regeneration of new collagen with a skin-firming effect. The clinical results are best assessed 3 to 4 months after the procedure, though most patients would notice improvements after about a month.
Botulinum toxin injection is the standard treatment for dynamic wrinkles – i.e., wrinkles that are worsened by facial animation. Effects usually last for 3 to 4 months. Mild bruising may be present at the needle entry sites. Clinical judgement needs to be exercised to deliver the optimal amount of toxin to alleviate wrinkles without causing an unnatural mask-like appearance.
Filler is used to replace volume; it can correct static deep facial folds (e.g., tear troughs and nasolabial folds) and contour deficits (e.g., sunken temporal areas), and can volumise the cheeks for a more youthful appearance. Filler provides an alternative for those patient who wants augmentation of the nasal dorsum without undergoing rhinoplasty. However, very rarely, the injection of filler into the nose can result in blindness or tissue necrosis. The chemical composition of fillers can be biological (e.g., hyaluronic acid or collagen) or synthetic (e.g., polytetrafluoroethylene). Synthetic fillers may last for more than a year but there is risk of infection and granuloma formation. In the interest of safety, shorter-acting filler material is preferable.
Botox and fillers complement each other, and some patients require both for optimal outcome.
INVASIVE (SURGICAL) PROCEDURES
Fat transfer (grafting) has gained much popularity over recent years as a method of volume replacement. Fat is a good filler option because it is autologous and contains a small amount of stem cells with rejuvenating properties. Fat grafting has been shown to improve the healing of post-irradiated chronic wounds. The final result is firmer skin with increased volume and improvement in wrinkles; the procedure may be repeated for a better cumulative result.
A thread lift procedure provides added levels of skin lifting to the cheeks and temporal area. Several threads made of absorbable material are inserted skin deep and stabilised by suturing to the temporal area. Swelling and bruising can last for a few weeks. The initial appearance may appear over-corrected; this normally improves over a few weeks to months. The clinical effects may last for one to two years.
Common surgeries for facial rejuvenation include blepharoplasty (eyelid surgery), brow lift, temporal lift, facelift and neck lift. These procedures can be done as a single procedure or as a combination, depending on the clinical state.
Upper eyelid surgery (blepharoplasty) can be done to create or improve the configuration of double eyelid or remove excessive droopy skin. It is therefore suitable for young patients who wish to create upper lid folds or older patients with droopy and puffy eyelids.
Ptosis (drooping) of the upper eyelid can co-exist with excessive skin. Not all patients with excess skin have ptosis. The various methods of ptosis correction depending on severity include levator plication or advancement, and in more severe cases something referred to as the FOOM flap.
Eyebags are caused by excessive fat accumulation and also laxity of skin and the orbital septum containing the bag of fat. Lower blepharoplasty can address both eyebags and excessive lower lid skin. There are two methods to remove eyebags: subciliary lower blepharoplasty (external method) and transconjunctival lower blepharoplasty (scarless method).
Subciliary lower blepharoplasty is suitable for patients with excess lower eyelid skin and fat pocket. Removal of fat would result in the gathering of excessive loose skin. Transconjunctival lower blepharoplasty is suitable for young patients with no skin laxity/ excess. The fat pocket is removed via a small cut in the back of the lower lid leaving no scar on the exterior.
A facelift and neck lift would address the problem of a sagging chin and jowl. The contour of the neck can be further improved by dividing the muscle band of the neck (platysmal band division for turkey neck deformity).
Endotine facelift is done via small incisions in the hairline, into which Endotine fixation devices are inserted. These are absorbable strips with small claws to lift up the cheek, jowl and neck. They are absorbed in about 3 to 6 months. Thus, Endotine lifting is suited for patients who do not have significant skin excess.
I often counsel patients that surgery to rejuvenate one area of the face may cause the neighbouring non-operated structure to appear out of sync. For example, in severe ageing eyelids, surgery to improve the eyebags without an upper eyelid procedures may cause the upper lid to appear slightly out of place. It is essential to understand that all features of the face age together. To achieve a harmonious appearance, a combination of procedures may need to be done simultaneously to address the various ageing features.
 Labiaplasty – Trim
Labiaplasty – Trim Labiaplasty – Wedge Excision
Labiaplasty – Wedge Excision Labiaplasty – Z Plasty
Labiaplasty – Z Plasty Labiaplasty – De-epithelialization
Labiaplasty – De-epithelialization Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis
Eye Cross Section – Double Eyelid – Blepharoplasty – Ptosis Blepharoptosis
Blepharoptosis Dermatochalasis
Dermatochalasis Blepharoptosis Assessment – MRD
Blepharoptosis Assessment – MRD Ptosis Assessment by Coverage of Limbus
Ptosis Assessment by Coverage of Limbus Blepharoptosis Assessment by MRD
Blepharoptosis Assessment by MRD Levator Function Test – Lid Closed
Levator Function Test – Lid Closed Levator Function Test – Lid Open
Levator Function Test – Lid Open Caucasian Double Eyelid vs Oriental Single Eyelid
Caucasian Double Eyelid vs Oriental Single Eyelid Suture Blepharoplasty
Suture Blepharoplasty Suture blepharoplasty – Cross section
Suture blepharoplasty – Cross section Incisional Blepharoplasty
Incisional Blepharoplasty Upper Eyelid – High Tapered fold – Blepharoplasty
Upper Eyelid – High Tapered fold – Blepharoplasty Upper eyelid – Parallel fold – Blepharoplasty
Upper eyelid – Parallel fold – Blepharoplasty Upper eyelid – Low in-fold – Blepharoplasty
Upper eyelid – Low in-fold – Blepharoplasty - Double eyelid surgery") Eyelid – Tapered fold (high)
Eyelid – Tapered fold (high)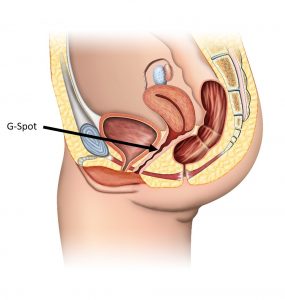 G-spot Location
G-spot Location Breast – Anatomy
Breast – Anatomy Silicone Breast Implant – Cohesive Gel
Silicone Breast Implant – Cohesive Gel Breast implant : Choice of Incisions
Breast implant : Choice of Incisions Breast implant – Sub-mammary placement
Breast implant – Sub-mammary placement Breast implant – Sub-pectoral placement
Breast implant – Sub-pectoral placement Abdominoplasty – Conventional Tummy Tuck
Abdominoplasty – Conventional Tummy Tuck Abdominoplasty – Mini Tummy Tuck
Abdominoplasty – Mini Tummy Tuck Abdominoplasty – Fleur de Lis
Abdominoplasty – Fleur de Lis Abdominoplasty – Belt
Abdominoplasty – Belt